ERcast: Clinical Perspectives Podcast Preview


Hippo ERcast January 2026
- Jan 2026
- 8 Chapters
- 2 hr 47 min
Welcome to the January 2026 Edition of ERcast! To kick off 2026, Drew and Andy review a 2025 study on the effects of private equity acquisition of hospitals. Brit Long discusses the evaluation and management of Multiple myeloma. Matt DeLaney and Tim Montrief tackle the real-world decision-making and the lifesaving complications of thrombolysis in the ED. Drew and Andy cover Intubations in the ED in 2025. Peds EM expert, Julia Magana, teases out the answer to the Prolonged Fever. Finally, Cam and Drew provide us with three articles to explore in Lit Matters. Enjoy!
Faculty
- Andy Little, DO
Dr. Andy Little is an emergency medicine physician and educator. He earned his medical degree from the Ohio University Heritage College of Osteopathic Medicine and completed his emergency medicine residency at OhioHealth Doctors Hospital Emergency Medicine Residency, where he served as Chief Resident. He has received multiple national awards, including recognition from the American Osteopathic Association, American College of Osteopathic Emergency Physicians, and Emergency Medicine Residents' Association.
- Cameron Berg, MD
Based in Minneapolis, MN, Dr. Berg focuses on simplifying complex patient care processes, such as chest pain, syncope, and heart failure treatment. Since 2020, he has also been navigating his own recovery from a TBI after a bicycle accident. When he isn't in the clinic, Cameron is usually busy keeping his three young children alive and happy.
- Drew Kalnow, DO
Dr. Drew Kalnow is an emergency medicine physician and educator based in Columbus, Ohio. He completed his emergency medicine training at OhioHealth Doctors Hospital Emergency Medicine Residency. Dr. Kalnow is passionate about advancing emergency medicine through high-quality education, with a particular focus on simulation, learning theory, and innovative teaching.
- Matthew DeLaney, MD, FACEP, FAAEM
Dr. Matthew DeLaney is an emergency medicine physician and educator based in Birmingham, Alabama. A native of Mobile, he earned his medical degree from the University of South Alabama and completed his emergency medicine residency at Maine Medical Center.Dr. DeLaney has experience in both community and academic emergency medicine and is known for his commitment to teaching and medical education. He lives in Birmingham with his wife, Erin, who is also a physician, and their two daughters.
- Brit Long, MD
Dr. Brit Long is a Professor of Emergency Medicine at the University of Virginia and an emergency medicine physician with experience in both a community ED and at a military academic center ED. He is the Clinical Editor-in-Chief of emDOCs.His professional interests include medical education, evidence-based medicine, and the FOAMed movement. Outside of work, he enjoys spending time with his wife and two daughters
- Tim Montrief MD, MPH
Dr. Timothy Montrief is an emergency medicine and critical care physician, educator, and author with interests in resuscitation, airway management, critical care, and medical education. He earned his MD and MPH degrees from the University of Miami Miller School of Medicine and completed his emergency medicine training at Jackson Memorial Hospital/University of Miami, followed by additional fellowship training in critical care medicine. Dr. Montrief has contributed extensively to emergency medicine education through academic publications, digital learning platforms, and FOAMed initiatives, including work with emDocs. His academic work has focused on critical care, ultrasound, toxicology, airway management, and high-risk emergency medicine presentations. Outside of medicine, he enjoys cooking, skydiving, and spending time near the ocean.
- Julia Magana, MD




Chapters
Private Equity Acquisition
Private equity acquisition of hospitals is associated with lower staffing, more interfacility transfers, and higher emergency department mortality. The signal in 2025 data is especially concerning for Medicare and Medicaid patients, with downstream effects that reach bedside throughput, ICU capacity, and local emergency care access. Private Equity and ED Outcomes Staffing cut signal: Private equity ownership was linked to lower salary spending across EDs and ICUs, a concrete marker of staffing contraction rather than simple accounting noise. Mortality impact: ED mortality rose from 52 to 60 deaths per 10,000 visits after acquisition, a 13% relative increase that makes this more than a finance story. Transfer burden: PE-owned hospitals transferred out more ED and ICU patients, consistent with shrinking in-house capacity and service line retrenchment. We get into what that looks like operationally in the episode. Capacity strain pattern: Shorter ICU stays appeared after acquisition, a directional sign of throughput pressure and reduced reserve capacity, though that finding was not statistically secure. Disproportionate patient impact: The harms appear to fall hardest on Medicare and Medicaid populations, reinforcing that ownership structure can widen existing access and outcome disparities. Emergency Physician Response Local advocacy role: Emergency physicians are often the first to see the downstream effects of service cuts, making local hospital committees and medical staff leadership important leverage points. State policy leverage: Regional and state advocacy matters because ownership-driven staffing changes and service closures often outpace what bedside clinicians can fix alone. Patient care framing: The core issue is not private equity as a label but whether profit-driven decisions erode staffing, capacity, and timely definitive care. Operational awareness: Rising transfers, thinner consultant coverage, and fewer staffed beds should be recognized as system signals, not isolated bad shifts. We lay out the practical implications on the show.
Thrombolytics for the Coding Patient
Cardiac arrest from suspected pulmonary embolism is one of the few code scenarios where thrombolytics remain a gestalt-driven decision. Bedside echo clues, bleeding risk, and post-ROSC hemorrhagic collapse all matter more than any single guideline line in PE-related PEA arrest. Thrombolytics in PE Cardiac Arrest Gestalt over hard evidence: No high-quality randomized data guide lytics in cardiac arrest from suspected PE, so the decision rests on pretest probability, bleeding risk, and whether thrombolysis could realistically change the outcome. PEA with RV clot: Witnessed PEA arrest with bedside echo showing RV strain or a right-heart thrombus is the classic high-suspicion picture that pushes clinicians toward alteplase despite the uncertainty. Guideline support remains weak: AHA/ACLS gives thrombolysis for confirmed or suspected PE arrest a Class IIb recommendation, which supports use but leaves substantial room for bedside judgment. Headline alteplase approach: Alteplase 50 mg IV push is a common arrest strategy, followed by ongoing CPR rather than immediate abandonment if pulses do not return right away. We get into the timing nuances in the episode. Mechanical CPR advantage: Mechanical CPR helps preserve team bandwidth during prolonged resuscitation after lytics, especially when the room also needs echo, airway management, and preparation for ROSC complications. Post-Lysis ROSC Deterioration Structured hemorrhage search: A patient who crashes after ROSC post-thrombolysis should trigger an organized search for bleeding, with a RUSH exam often serving as the first bedside screen. Ultrasound first look: RUSH helps rapidly assess RV and LV function, IVC caliber, and pericardial effusion while also steering you toward hemorrhagic versus obstructive or cardiogenic shock. Occult bleeding patterns: Hemothorax, intra-abdominal hemorrhage, and retroperitoneal bleeding are the big post-lysis misses when a patient initially appears stable and then decompensates. Escalation beyond ultrasound: If bedside ultrasound is unrevealing and instability persists, cross-sectional imaging of the chest, abdomen, and pelvis may be necessary to find the source. We walk through that escalation in the chapter. Reversal is targeted: TPA reversal is reserved for major bleeding, with cryoprecipitate aimed at fibrinogen repletion and tranexamic acid used to blunt ongoing fibrinolysis. PCC practical pearl: Four-factor PCC is a favored rapid adjunct when urgent reversal is needed, while large-volume plasma can be problematic in patients already struggling with RV failure.
Lit Matters #1: HFNC vs NIV in Acute Exacerbations of COPD
Acute exacerbation of COPD with moderate hypercapnic respiratory failure is still a noninvasive ventilation problem, not a high-flow nasal cannula problem. In this randomized non-inferiority trial, HFNC did not match NIV for treatment failure or intubation, even though comfort and skin tolerance favored HFNC. HFNC versus NIV in AECOPD First-line modality choice: NIV remains the standard initial support for AECOPD with acute hypercapnic respiratory failure because HFNC failed its non-inferiority test and showed more treatment failures overall. Treatment failure signal: The primary endpoint favored NIV, with treatment failure driven by persistent CO2 retention and respiratory distress rather than a simple comfort issue. Intubation risk difference: HFNC was associated with a notably higher intubation rate, a concrete reminder that better comfort does not equal equivalent ventilatory support. Physiology of support: HFNC offers humidification, dead-space washout, and some positive pressure, but obstructive physiology still responds better to the ventilatory unloading NIV provides. Comfort versus efficacy: HFNC caused less skin breakdown and needed fewer airway-care interventions, making it a reasonable backup when NIV is not tolerated. We get into practical NIV-comfort strategies in the episode. Applicable patient window: These results apply to moderate hypercapnic COPD exacerbations with respiratory acidosis, not the crashing patient who needs immediate intubation or the severe acidosis group excluded from the trial.

The Prolonged Fever
Most prolonged fever in healthy, vaccinated children is still viral, and common respiratory viruses can run up to 8 days. In pediatric fever without a source, the key ED question is when duration, exam findings, and vaccination status justify a broader workup for bacterial, inflammatory, or malignant causes. Approach to Prolonged Pediatric Fever Typical viral fever timeline: Benign viral illnesses usually resolve by day 3 to 5, but adenovirus, influenza, RSV, COVID, and EBV can keep children febrile for as long as 8 days. Prolonged fever definition: There is no single cutoff, but most pediatric studies call fever beyond 5 to 7 days prolonged, while fever of unknown origin usually extends past 10 to 14 days. History and exam first: A careful exposure history and focused physical exam do more than broad screening panels to separate a lingering virus from UTI, pneumonia, Kawasaki disease, or malignancy. Laboratory workup trigger: For a well-appearing child, labs become more reasonable once fever passes 7 days, with CBC, inflammatory markers, urinalysis, and selected cultures forming the usual starting point. We walk through what makes that trigger move earlier in the episode. Vaccination status matters: Occult bacteremia in immunized children with fever without a source is under 1%, while pre-vaccine era estimates were 3% to 11%, making under-immunization a meaningful risk shift. Serious infection prevalence: In children with fever lasting at least 5 days, serious bacterial infection remains uncommon at 8.4%, and most cases are still UTI or pneumonia rather than meningitis or another invasive infection. Red Flags, Differential, and Disposition Bacterial source clues: UTI is the most common nonviral cause of pediatric fever, and fever above 104 F should raise suspicion for a bacterial source even though temperature alone does not define severity. Inflammatory disease signals: Prolonged fever plus rash, joint swelling, mucous membrane changes, or lymphadenopathy should shift the differential toward Kawasaki disease, lupus, juvenile idiopathic arthritis, or inflammatory bowel disease. Malignancy warning signs: Weight loss, headaches, or abnormal bruising and bleeding are the classic concerning companions to prolonged fever, though occasionally fever is the only early clue. Persistent tachycardia concern: Tachycardia that persists despite hydration deserves a wider search for myocarditis, pericarditis, or other serious illness, with ECG and troponin as targeted next tests. Antipyretic treatment framing: Fever itself is usually physiologic rather than harmful, so treatment is driven by comfort and hydration; tachypnea, diaphoresis, lethargy, and even hallucinations often improve after antipyresis. Admission versus discharge: Ill appearance, poor oral intake, inability to walk, high inflammatory markers, or unreliable follow-up all push toward admission, while pending blood cultures can be managed outpatient in selected children. The follow-up handoff details are worth hearing in the chapter.

Intubate like it’s 2025
Emergency tracheal intubation still carries major peri-intubation risk, with hypoxemia and hypotension remaining common complications. Current ED airway evidence favors positive-pressure preoxygenation, routine video laryngoscopy, and using either a stylet-loaded endotracheal tube or a bougie rather than a bare tube. Evidence-Based ED Intubation Positive-pressure preoxygenation: Noninvasive ventilation is now the preferred preoxygenation strategy when feasible, cutting hypoxemia and even lowering peri-intubation cardiac arrest compared with oxygen delivery that does not provide positive pressure. Bag-mask during induction: Ventilation between induction and laryngoscopy reduces hypoxemia without increasing aspiration, making bag-mask support a default move rather than something to avoid reflexively, and we get into the setup details in the episode. Limited role for apneic oxygenation: Routine nasal-cannula or high-flow apneic oxygenation has not improved nadir oxygen saturation or reduced hypoxemia during laryngoscopy, so it should not be treated as a cornerstone maneuver. RSI medication fab four: For standard ED rapid sequence intubation, etomidate or ketamine for induction and succinylcholine or rocuronium for paralysis remain the practical first-line choices; familiarity is the deciding principle. Post-intubation hypotension readiness: Peri-intubation hypotension is driven by vasodilation, loss of catecholamine tone, and reduced venous return under positive pressure, and prophylactic fluid boluses have not prevented it in normotensive patients. Video plus introducer strategy: Video laryngoscopy outperforms direct laryngoscopy even in contaminated airways, and first-pass technique should include either an endotracheal tube with stylet or a bougie. We walk through why the bare tube should be retired in the chapter.

Lit Matters #2: 2025 GOLD Report updates
COPD exacerbation severity can now be graded at first contact rather than inferred from the treatment you end up giving. The 2025 GOLD update also pushes emergency clinicians to think beyond “just COPD,” with tighter steroid and antibiotic courses, earlier NIV for respiratory failure, and more attention to cardiovascular overlap. COPD Exacerbation Assessment and Management Rome severity proposal: The Rome proposal classifies COPD exacerbations at the bedside using dyspnea burden, vital signs, oxygen saturation, and CRP, giving ED teams a real-time triage framework. We walk through the practical cut points in the episode. Severe exacerbation definition: Severe exacerbation means the clinical criteria are met plus acute hypercapnic respiratory failure with acidosis, anchoring ICU-level concern to the blood gas rather than to how much treatment has been given. Short steroid course: Prednisone 40 mg daily for 5 days remains the headline systemic steroid regimen, with better lung function and faster recovery but no proven benefit from extending the course. Antibiotic trigger symptoms: Antibiotics belong when Anthonisen features are present, especially increased sputum purulence paired with more dyspnea or sputum volume, and the recommended course is just 5 days. Avoid methylxanthines: Theophylline and other methylxanthines are explicitly not recommended in acute exacerbations because the adverse-effect burden outweighs any marginal bronchodilator benefit. NIV before intubation: Noninvasive ventilation is first-line for COPD patients with acute respiratory failure, especially respiratory acidosis, because it lowers intubation rates, shortens length of stay, and improves survival. Cardiovascular Overlap and Prevention Broader dyspnea differential: Worsening respiratory symptoms are not specific for COPD; pneumonia, acute heart failure, and pulmonary embolism stay near the top of the ED differential when the story does not quite fit. COPD cardiovascular syndemic: GOLD frames COPD and cardiovascular disease as a syndemic, with shared risk factors and bidirectional worsening that raises concern for MI and arrhythmias during and after exacerbations. Cardiac biomarker role: Troponin and BNP may help during a presumed COPD exacerbation when ischemia or heart failure is in the differential or the response to standard therapy is unexpectedly poor. Discharge vaccine updates: Exacerbation prevention now includes RSV vaccination for older adults and patients with chronic heart or lung disease, alongside annual influenza, pneumococcal PCV20 or PCV21, and Tdap.
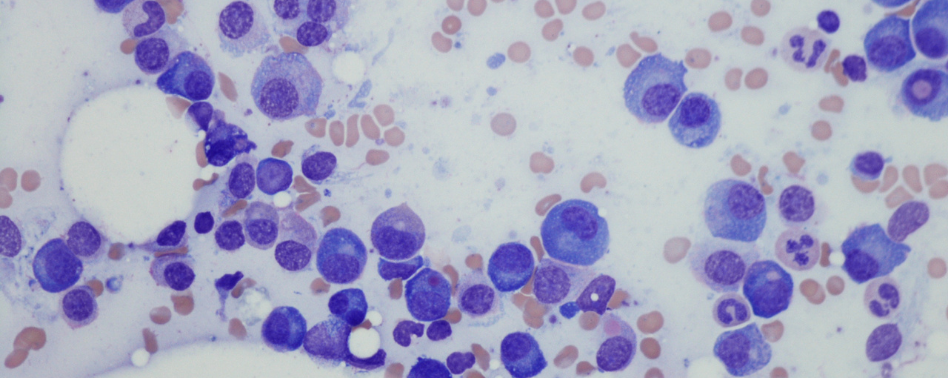
Multiple Myeloma
Multiple myeloma often first declares itself in the ED through organ injury rather than a known cancer diagnosis. CRAB findings—hypercalcemia, renal dysfunction, anemia, and bone lesions—should sharpen suspicion, especially when anemia, acute kidney injury, and hypercalcemia cluster together. Recognizing Multiple Myeloma in the ED CRAB complication pattern: Hypercalcemia, renal dysfunction, anemia, and bone lesions are the classic bedside clues, and the combination of anemia with acute kidney injury or hypercalcemia should prompt a myeloma workup. Typical initial presentations: Unexplained anemia is the most common presenting feature, with bony pain, acute kidney injury, fatigue, weight loss, and hypercalcemia rounding out the usual emergency-department picture. High-yield ED testing: CBC, BMP, and ionized calcium are the key emergency tests, with ionized calcium being unusually helpful here because total calcium can mislead in clinically important myeloma hypercalcemia. Definitive diagnosis pathway: Urine protein electrophoresis and bone marrow biopsy establish the diagnosis, but the emergency task is recognizing the complication pattern early enough to trigger the right downstream evaluation. We get into that diagnostic handoff in the episode. Imaging for bone pain: Plain radiographs are the starting point for focal bony pain, while CT can better define lytic lesions and structural risk when a pathologic process is already on the table. Major Myeloma Complications and Management Renal injury burden: Acute kidney injury is common, with creatinine often already above 2 mg/dL at diagnosis, and supportive care matters because kidney dysfunction is reversible in a meaningful share of patients. Hypercalcemia framing: Myeloma hypercalcemia is driven by bone demineralization, and severe cases are treated with IV fluids, calcitonin, and a bisphosphonate, with dialysis sometimes needed for the sickest patients. Infection risk window: Infection risk is markedly elevated—about 7- to 11-fold higher than the general population—and is highest early in treatment, so sepsis coverage should be broad and early, with antivirals added when viral disease is plausible. Skeletal instability clues: Osteolytic disease is present in roughly 70% of patients, and pathologic or insufficiency fractures are common enough that any fracture in suspected myeloma deserves a more careful imaging strategy. We walk through when to escalate imaging in the chapter. Spinal cord red flags: Nerve root compression is the most important neurologic complication, and cauda equina syndrome makes MRI and urgent specialty involvement time-critical. Therapy-related thrombosis: Myeloma carries a strikingly elevated VTE risk, especially in the first 6 months of therapy, and confirmed DVT or PE is generally treated with LMWH or a DOAC.
Lit Matters #3: 2025 ATS CAP Guidelines Update
Community-acquired pneumonia now reflects host susceptibility, lung microbiome dysbiosis, and alveolar inflammation rather than simple invasion of a sterile lung. The 2025 ATS update shifts CAP care toward ultrasound-supported diagnosis, selective antibiotics after a positive viral PCR, shorter courses once patients are clinically stable, and steroids only in the right inpatient phenotype. 2025 CAP Guideline Practice Shifts Lung ultrasound diagnosis: Lung ultrasound is an acceptable alternative to chest radiography for suspected CAP when operator expertise exists, and it may help when chest x-ray is negative but suspicion remains high. Positive viral PCR context: A positive respiratory viral panel does not reliably exclude bacterial coinfection, so empiric antibiotics are generally withheld only in otherwise healthy outpatients without comorbidities. Clinical stability shortening: Antibiotic duration can be shorter than 5 days for stable outpatients and selected non-severe inpatients, but severe CAP still generally needs at least 5 days. We get into the stability criteria in the episode. Severe CAP steroids: Systemic corticosteroids are not recommended for non-severe inpatient CAP, but severe CAP is different, with an estimated 1 death prevented for every 17 treated patients. Influenza caution: Severe influenza pneumonia remains an important exception because observational data suggest corticosteroid harm, even as steroids may help in other severe CAP phenotypes. CAP Pathophysiology And Bedside Judgment Modern CAP model: CAP is better framed as dysbiosis, inflammation, and tissue injury in a susceptible host, which helps explain why microbiology, imaging, and treatment decisions rarely fit a single rule. Imaging confirms disease: CAP diagnosis still requires compatible symptoms plus chest imaging showing alveolar inflammation; clinical impression alone is not enough to establish the diagnosis. Coinfection uncertainty: No clinical, radiographic, or laboratory test can reliably separate viral pneumonia from bacterial coinfection, which is why viral PCR results must be interpreted in context. Long course harms: Prolonged antibiotic therapy carries real downside, including C difficile, acute kidney injury, adverse drug effects, and microbiome disruption, without clear benefit in stable patients. Exceptions to shortcuts: Short courses and simplified pathways do not apply cleanly to necrotizing infection, abscess, empyema, resistant organisms, or major chronic lung disease. We cover the important caveats on the show. Patient Communication In CAP Recommendation rationale: Good CAP communication starts with why a test or treatment is being recommended, using plain language that links the plan to the patient's illness and priorities. Certainty and tradeoffs: Patients should hear how strong the recommendation is and the main tradeoffs, including side effects, cost, convenience, and the risk of undertreating or overtreating infection. Expected clinical course: Set expectations for recovery, follow-up, and return precautions early, because realistic timelines and warning signs are part of safe outpatient and inpatient CAP care. Shared follow-up planning: Clear instructions on how to contact the team and arrange follow-up are part of the treatment plan, especially when antibiotics are withheld or shortened.