ERcast: Clinical Perspectives Podcast Preview


Hippo ERcast February 2023
- Feb 2023
- 7 Chapters
- 2 hr 34 min
This February 2023 edition of ERCAST starts with Matt and Drew talking about what constitutes physician impairment and how to identify available resources. Next up, Drew sits down with wilderness expert, Geoff Comp, to describe cold weather-related conditions, treatment strategies, and special considerations. Sara Gray and Drew discuss how, when, and when not to use HFNC. Andy and Reuben Strayer dive into the uses and pitfalls of the various tools available in cases of syncope. DeLaney and Lauren Westafer dig deeper into pulse checks and why this common practice probably needs to be put to rest. Finally, Tiffany Proffitt discusses the most common bleeding ENT emergencies. Enjoy!
Faculty
- Drew Kalnow, DO
Dr. Drew Kalnow is an emergency medicine physician and educator based in Columbus, Ohio. He completed his emergency medicine training at OhioHealth Doctors Hospital Emergency Medicine Residency. Dr. Kalnow is passionate about advancing emergency medicine through high-quality education, with a particular focus on simulation, learning theory, and innovative teaching.
- Matthew DeLaney, MD, FACEP, FAAEM
Dr. Matthew DeLaney is an emergency medicine physician and educator based in Birmingham, Alabama. A native of Mobile, he earned his medical degree from the University of South Alabama and completed his emergency medicine residency at Maine Medical Center.Dr. DeLaney has experience in both community and academic emergency medicine and is known for his commitment to teaching and medical education. He lives in Birmingham with his wife, Erin, who is also a physician, and their two daughters.
- Tiffany Proffitt, DO
Dr. Proffitt is a board-certified Emergency Medicine physician practicing in Scottsdale, Arizona. She completed her medical training at Midwestern University Chicago College of Osteopathic Medicine and found her passion for medical education during her residency at Spectrum Health Lakeland. Tiffany is the co-founder and co-chairwoman of the HonorHealth Women Physicians Leadership Council, where she works to enhance professional development for 550 women clinicians. When she isn’t in the ED or podcasting, she’s chasing twins, dancing with toddlers, and enthusiastically singing the wrong lyrics to every song.
- Andy Little, DO
Dr. Andy Little is an emergency medicine physician and educator. He earned his medical degree from the Ohio University Heritage College of Osteopathic Medicine and completed his emergency medicine residency at OhioHealth Doctors Hospital Emergency Medicine Residency, where he served as Chief Resident. He has received multiple national awards, including recognition from the American Osteopathic Association, American College of Osteopathic Emergency Physicians, and Emergency Medicine Residents' Association.
- Geoffrey Comp, DO, FACEP
Dr. Comp is an Associate Program Director for the Creighton University / Valleywise Health Emergency Medicine Residency Program in Phoenix. A clinician-educator at heart, Geoff spends his time mentoring the next generation of Emergency Medicine residents and advocating for better ways to teach and learn medicine. His professional world revolves around wilderness medicine, clinician wellness, and finding innovative ways to bridge the gap between theory and the bedside. When he isn’t in the ED or the classroom, you’ll likely find him combining his love for medicine with his passion for the outdoors, always looking for a new trail to explore or a new way to collaborate with fellow clinicians.
- Lauren Westafer, DO, MPH, MS
- Reuben Strayer, MD
- Sara Gray, MD




Chapters
The Impaired Clinician
Physician impairment is a functional patient-safety problem, not a synonym for mental illness, substance use disorder, or disability. The key question is whether a clinician’s current condition is impairing judgment, competence, or professional performance, and major physician-health programs are built to support treatment without reflexive punishment. Recognizing and Responding to Physician Impairment Impairment versus diagnosis: A health problem alone does not equal impairment; the defining issue is whether current symptoms or behaviors make a clinician unable to provide safe, competent patient care. Functional safety standard: The practical test is present-tense performance: impaired judgment, ethical lapses, or degraded clinical reliability matter more than a past diagnosis or treatment history. Alcohol use example: Alcohol dependence after shifts is not automatically reportable impairment if the physician is practicing safely, which is exactly the distinction many clinicians blur under stress. Approaching a colleague: When you suspect unsafe practice, act on the patient-safety concern and connect the clinician to a Physician Health Program rather than trying to adjudicate the whole situation alone. We get into the wording for that conversation in the episode. Supportive policy protections: ACEP explicitly states that voluntarily stepping back from practice, getting treatment, or requesting a required disability accommodation should not trigger retaliation or disciplinary action. Licensing question reform: ACEP argues licensing and credentialing should focus on current untreated impairment, not prior diagnosis or treatment, and even offers a better model question for boards and hospitals.
Cold Weather Blues: Hypothermia
Accidental hypothermia is a systemic emergency marked by progressive neurologic depression, cold diuresis, and escalating cardiac instability as core temperature falls. Management is driven more by symptoms than by the thermometer, and severe cases can deteriorate into refractory ventricular fibrillation with minimal movement. Hypothermia Recognition and Physiology Primary versus secondary causes: Not all hypothermia comes from outdoor exposure; sepsis, intoxication, hypothyroidism, adrenal insufficiency, shock, and malnutrition can all impair thermoregulation and change the workup. Symptom based severity: Clinical status matters more than the exact core temperature: shivering and intact mentation suggest milder disease, while lethargy, coma, and loss of shivering mark dangerous progression. We lay out the bedside staging in the episode. Shivering physiology shift: Physiology rises early with cold stress, but around 30 C shivering stops and metabolism falls, removing the patient's main endogenous heat source and accelerating decompensation. Cold diuresis and hypovolemia: Hypothermic patients are often intravascularly depleted from cold-induced diuresis, plasma shift, and poor intake, which helps explain hypotension and the need for volume repletion. Cardiac irritability threshold: Below 30 C, the myocardium becomes exquisitely prone to refractory ventricular fibrillation, triggered by movement, acidosis, hypocarbia, or hypoxia. ED Management and Cardiac Arrest Immediate ED priorities: Start with rewarming, a STAT fingerstick glucose, ECG, and basic labs including coagulation studies; if the cause is unclear, broaden quickly to endocrine, infectious, and toxicologic testing. Electrocardiographic warning signs: Expect early tachycardia followed by bradycardia that is often atropine-refractory, with PR, QRS, and QT prolongation; Osborn waves may appear below 30 C. Rewarming strategy tiers: Passive external, active surface, warmed IV fluids, heated humidification, cavity lavage, and ECMO all have roles, but the choice depends on instability and available resources. We get into the escalation logic in the chapter. Medication and shock caution: Drug metabolism slows in severe hypothermia, so repeat doses can accumulate; mild hypotension often improves with rewarming, while vasopressors are reserved for selected patients. Defibrillation and pulse checks: Serial shocks for VT or VF are often low yield until rewarming advances, and peripheral pulses can be misleading enough that ultrasound or an arterial line may be more trustworthy. Termination of resuscitation: Hypothermic arrest can still have good neurologic outcomes, so resuscitation generally continues until meaningful rewarming, with a very high potassium level serving as a grave prognostic marker.
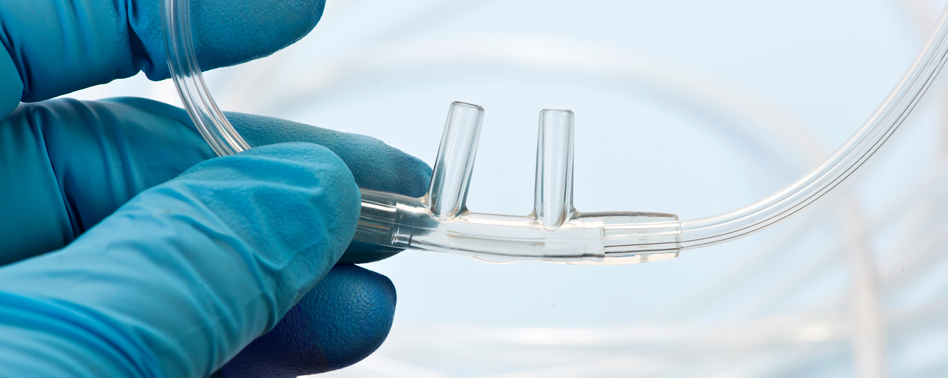
High Flow Hacks, Part 1
High-flow nasal cannula is an oxygenation strategy for acute hypoxemic respiratory failure, not a substitute for ventilatory support. HFNC improves comfort, allows eating and speech, and can buy time safely when paired with reassessment tools like the ROX index. High-Flow Nasal Cannula Basics Best-fit respiratory failure: HFNC fits acute hypoxemic respiratory failure, especially when patients need high FiO2 without the mask burden of traditional noninvasive ventilation. Device physiology and comfort: Heated humidified flow up to 50-60 L/min reduces air hunger and improves tolerance, while allowing patients to talk, eat, and clear secretions. Low-level PEEP effect: HFNC generates a modest PEEP effect at higher flows, most noticeable when the patient keeps the mouth closed, a bedside trick we emphasize in the episode. Ideal bedside candidates: Good candidates include septic hypoxemia, secretion-heavy or vomiting patients, claustrophobia with masks, and preoxygenation before intubation. Escalation mindset early: If you are approaching the ceiling of your device, think ahead to intubation rather than reflexively stepping to NIV unless the diagnosis has changed. Choosing HFNC Versus NIPPV Oxygenation versus ventilation: HFNC is primarily an oxygenation tool, whereas BiPAP adds inspiratory support and unloads work of breathing in mechanical respiratory failure. COPD and CHF exception: BiPAP remains the preferred noninvasive strategy for COPD and cardiogenic pulmonary edema, where mortality benefit is already established. CPAP versus BiPAP distinction: CPAP supplies continuous pressure like PEEP, while BiPAP adds separate inspiratory pressure support that better assists the tiring patient. Tolerance rescue options: Mask intolerance should start with verbal coaching; if needed, tiny-dose ketamine or fentanyl can help, with nuances on patient selection we get into in the chapter. When to intubate: Worsening hypoxia, rising work of breathing, aspiration risk, declining mental status, or arrest are hard stops where noninvasive support has failed. Predicting HFNC Failure ROX index role: The ROX index combines oxygenation with respiratory rate and is the most ED-friendly way to track whether HFNC is working or failing. Trend over time: A ROX index that stays low or worsens over serial checks signals likely failure; we walk through the timing checkpoints in the episode. P/F ratio limits: A falling P/F ratio also points to worsening lung injury, but repeated ABGs and longer observation make it less practical in the ED. Severity score signal: Higher or rising SOFA and APACHE scores correlate with HFNC failure, though they are usually too cumbersome for real-time emergency decisions. Delayed intubation risk: The real hazard is not HFNC itself but missing failure early, because delayed intubation in worsening hypoxemia is linked to worse outcomes.

Done Fell Out: Is There a Role for Syncope Scores in the ED?
Syncope admissions are common, but truly actionable bad outcomes after admission are rare. In ED syncope evaluation, no major risk score has consistently outperformed clinician gestalt, so disposition is better driven by a structured workup for arrhythmic, structural, traumatic, and noncardiac causes. Syncope Scores and Their Limits Low-yield admission reality: Most admitted syncope patients never undergo an intervention, and adverse outcomes occur in less than 1%, which is why reflex admission based on fear alone performs poorly. Gestalt versus formal scores: The San Francisco Syncope Rule and Canadian Syncope Risk Score have not consistently beaten physician judgment, a useful reality check when a number feels more objective than it is. Multi-system syndrome problem: Syncope is a presentation, not a single disease, so collapsing arrhythmia, hemorrhage, reflex syncope, seizure mimic, and trauma into one score predictably loses bedside nuance. Guideline role in disposition: Risk tools and the 2017 AHA approach can still support shared decision-making, but only after the dangerous causes have been actively considered. We get into that sequencing in the episode. Presyncope clinical equivalence: Near-syncope should generally be treated as the same or a very similar disease process as true syncope, especially when the story raises concern for cardiac pathology. Structured ED Syncope Evaluation Resuscitation first principle: Start with ABCs and vital signs because syncope with hypotension, hypoxia, or persistent instability is not a scoring problem but a resuscitation problem. Trauma double-focus: Falls can hide intracranial injury or fracture, but the opposite miss matters too: obvious trauma can distract from the underlying cause of syncope that triggered it. ECG-centered danger screen: History, exam, and ECG remain the core triad, with special attention to arrhythmic and structural red flags rather than a broad shotgun lab strategy. Cause-based diagnostic framing: A practical workup asks what happened and what is happening now: seizure mimic, noncardiac dangerous causes, cardiac syncope, and benign reflex or orthostatic etiologies. Safety capital and follow-up: Disposition depends partly on whether the patient can recognize worsening, return promptly, and succeed with outpatient care rather than on a score alone. Common Syncope Workup Pitfalls Routine head CT overuse: Brain imaging is usually not indicated unless there is concerning head trauma or a focal neurologic finding, a high-yield restraint point in syncope workups. Pulmonary embolism overtesting: PE should be assessed with usual history-and-exam risk stratification, not routinely excluded with D-dimer or CT angiography just because the patient fainted. Orthostatic vitals trap: Orthostatic changes do not reliably guide management because orthostasis is a physiologic finding with multiple possible causes, not a final diagnosis. Troponin interpretation nuance: Troponin helps mainly when it is positive; a normal value does little for undifferentiated syncope because arrhythmia often causes no troponin rise. That distinction is worth hearing in the chapter.
High Flow Hacks, Part 2
High-flow nasal cannula is a humidified, high-flow oxygen strategy for acute hypoxemic respiratory failure, not a replacement for BiPAP in hypercapnic COPD or cardiogenic pulmonary edema. The key bedside question is who will improve on HFNC and who is declaring early failure. High-Flow Nasal Cannula Basics Best-fit clinical phenotype: HFNC fits acute hypoxemic respiratory failure, especially when patients need high FiO2 but would benefit from a nasal interface they can tolerate while talking, eating, or clearing secretions. Physiology of high flow: Flow does more than deliver oxygen: heated humidification improves comfort, high rates wash out dead space, and a closed mouth can generate a modest PEEP effect of about 1 cm H2O per 10 L/min. Initial bedside targets: Set FiO2 to an SpO2 of 92-96%, use 37 C for humidification, and titrate flow to visible work of breathing rather than treating the liters per minute as a fixed number. Situations favoring HFNC: HFNC is particularly useful for sepsis, secretion-heavy patients, mask intolerance, and preoxygenation before intubation. We get into the setup nuances in the episode. When HFNC is wrong tool: HFNC does not provide the inspiratory pressure support that mechanical respiratory failure needs, so COPD exacerbations and CHF remain classic BiPAP territory with known mortality benefit. Recognizing HFNC Failure Early ROX index trend: The ROX index combines oxygenation with respiratory rate and is the most practical ED tool for tracking HFNC success versus looming intubation, with serial checkpoints that matter. We walk through the timing nuances in the episode. Worsening oxygenation markers: A falling P/F ratio signals worsening lung injury, but it is less ED-friendly because it usually requires repeated ABGs and trend data over hours rather than a quick bedside reassessment. Severity score context: Rising SOFA or APACHE scores correlate with HFNC failure, but they are cumbersome for real-time emergency care and should not distract from the patient's trajectory at the bedside. Escalation ceiling awareness: Maxing out HFNC should trigger parallel planning for intubation, because delayed recognition of failure can worsen outcomes in acute hypoxemic respiratory failure. Noninvasive step after HFNC: Switching from HFNC to BiPAP is usually not the next best move unless the original diagnosis was wrong and the patient actually has a pressure-support problem such as COPD or CHF. BiPAP, CPAP, and Intubation Thresholds CPAP versus BiPAP distinction: CPAP is continuous positive pressure, while BiPAP adds inspiratory support akin to pressure support ventilation, making it the more common ED choice when work of breathing is high. Mortality-benefit indications: BiPAP remains the evidence-based first-line noninvasive strategy for COPD and acute CHF, where inspiratory assistance and positive pressure improve more than oxygenation alone. Tolerance without oversedation: Start with verbal de-escalation, avoid benzodiazepines, and if needed use small-dose ketamine or fentanyl cautiously because preserving respiratory drive and hemodynamics is the whole game. Hemodynamic PEEP caution: PEEP recruits alveoli and improves VQ matching, but it can also reduce preload in a dose-dependent way, a key hazard when initiating positive pressure in cardiogenic shock. Signals to intubate now: Worsening hypoxia, rising work of breathing, aspiration risk, falling mental status, or arrest are hard stops for noninvasive support. That bedside pivot is worth hearing in the chapter.

Is it Time to Pause Pulse Checks?
High-quality CPR depends on minimizing interruptions, and routine pulse checks are a surprisingly common source of avoidable pause time. In cardiac arrest care, rhythm checks every 2 minutes align better with current ACLS thinking, while POCUS should answer a focused question without stopping compressions. CPR Interruptions and Pulse Checks Chest compression fraction: Chest compression fraction tracks how much of the resuscitation is spent actually compressing the chest, and higher fractions are linked to better ROSC and functional outcomes. Pulse check inaccuracy: Manual pulse checks are both slow and unreliable, with studies showing 17 to 24 seconds to decide and accuracy around 78%, making them a poor trade for lost compression time. Guideline shift away: AHA guidance has moved away from routine pulse checks during CPR, even for presumed ROSC, while keeping the emphasis on near-continuous compressions. Rhythm check priority: Rhythm checks every 2 minutes identify actionable rhythms like VF or VT for defibrillation, and asystole does not require a pulse check before CPR continues. That practice change is worth hearing in the episode. Arterial line exception: An arterial line can help confirm perfusion in the right patient, but it does not change the larger bedside principle that routine pulse palpation should stop. POCUS During Cardiac Arrest Ultrasound pause penalty: POCUS during arrest is associated with longer CPR pauses, and transthoracic scans commonly push interruptions beyond the 10-second target. TEE over TTE: Transesophageal echo shortens compression pauses compared with transthoracic imaging, with reported pauses of 9 seconds versus 19 seconds. Targeted ultrasound question: Ultrasound should start with a specific diagnostic question, with image capture kept brief and interpretation handed off while compressions continue. We get into that workflow in the episode. CPR first principle: POCUS can add useful information during resuscitation, but it should never delay ongoing high-quality CPR or become the reason compressions stop.
A Face Full of Blood: ENT Tips and Tricks
ENT bleeding emergencies are airway and hemorrhage problems first: post-tonsillectomy hemorrhage can escalate fast, auricular hematoma can destroy cartilage within 24 hours, and most tongue lacerations heal without sutures. Epistaxis, peritonsillar abscess, and dental bleeding all reward a few precise bedside moves. Tongue lacerations and oral bleeding Selective tongue closure: Tongue lacerations under 2 cm that are non-gaping at rest and spare the tip usually heal well by secondary intention, with no functional or cosmetic advantage from routine suturing. High-yield wound exam: Look for tooth fragments, other intraoral injuries, and signs of hemorrhage or airway compromise before focusing on closure; those associated injuries matter more than the tongue itself. Primary repair triggers: Persistent bleeding, bisecting wounds, large flaps, tip involvement, and larger gaping lacerations are the main reasons to close rather than observe. We get into the bedside judgment calls in the episode. Sedation-aware repair: When closure is needed, a larger absorbable suture such as 2-0 or 3-0 is preferred, and many children need referral for procedural sedation rather than a rushed repair. Dental socket hemostasis: Post-dental bleeding often stops with 20 minutes of direct pressure on gauze, with lidocaine-epinephrine, TXA, or thrombin as useful topical adjuncts, especially in anticoagulated patients. Post-tonsillectomy hemorrhage Delayed bleed window: Secondary post-tonsillectomy hemorrhage classically appears around days 7 to 10 when the fibrin eschar separates, and even a minor bleed can evolve into major hemorrhage. Lateral pressure technique: Apply pressure laterally against the tonsillar fossa vessels rather than pushing straight posteriorly; that simple directional change can improve control while help is mobilized. Airway-first setup: Keep the patient leaning forward with suction ready, and call ENT plus anesthesia early because these cases can deteriorate into difficult airway management without much warning. Adjunct hemostatic options: Ice water, TXA, racemic epinephrine, and in selected children DDAVP are reasonable temporizing therapies for ongoing bleeding, with route and sequencing nuances we walk through in the episode. Intubation red flags: Severe active hemorrhage and any sign of airway compromise should push the team toward definitive airway planning early rather than repeated bedside attempts at local control. Peritonsillar abscess, epistaxis, and ear hematoma PTA imaging choice: CT with IV contrast is highly sensitive for peritonsillar abscess and especially useful with severe trismus, while ultrasound can confirm the collection and define nearby anatomy. PTA drainage target: Needle aspiration is aimed at the superior pole with careful controlled passes under direct visualization, followed by antibiotics and ENT follow-up within 48 hours. Anterior packing basics: For epistaxis that persists after pressure, have the patient clear clots before placing an anterior pack such as a Rhino Rocket, but avoid it with nasal fracture or septal perforation. Timed epistaxis reassessment: A formal recheck after 15 to 20 minutes matters because apparent hemostasis can be misleading once the pack is partially deflated. We cover the practical reassessment sequence in the chapter. Auricular hematoma urgency: Auricular hematoma is a perichondrial separation injury that can progress to cartilage necrosis and cauliflower ear within 24 hours, so drainage should not wait. Compression after drainage: Evacuation alone is not enough; a dental-roll bolster or compression dressing must eliminate dead space, with anti-staphylococcal coverage and ENT follow-up to prevent reaccumulation.