ERcast: Clinical Perspectives Podcast Preview
The summary below is from an episode of ERcast: Clinical Perspectives
Posterior reversible encephalopathy syndrome is a neuroimaging diagnosis defined by acute neurologic symptoms plus vasogenic edema, often in the setting of severe hypertension. Normal head CT does not exclude PRES, and early treatment centers on controlled blood pressure reduction, seizure control, and trigger reversal.
Recognizing PRES in the ED
- Core diagnostic picture: PRES is acute headache, seizure, vision change, or altered mental status paired with vasogenic edema on imaging; hypertension is common but a normal blood pressure does not rule it out.
- High-yield risk factors: Severe hypertension drives 50-90% of cases, and the syndrome is also linked to eclampsia, renal failure, autoimmune disease, transplant, and drugs like immunosuppressants or linezolid.
- Typical symptom pattern: Seizures are especially common, occurring in roughly 75% of cases, with altered mental status and visual symptoms rounding out the classic emergency department presentation.
- Why PRES happens: The pathophysiology is a mix of failed cerebral autoregulation, endothelial dysfunction, and focal vasoconstriction, which together produce vasogenic rather than cytotoxic edema. We get into the bedside implications in the episode.
Imaging and initial management
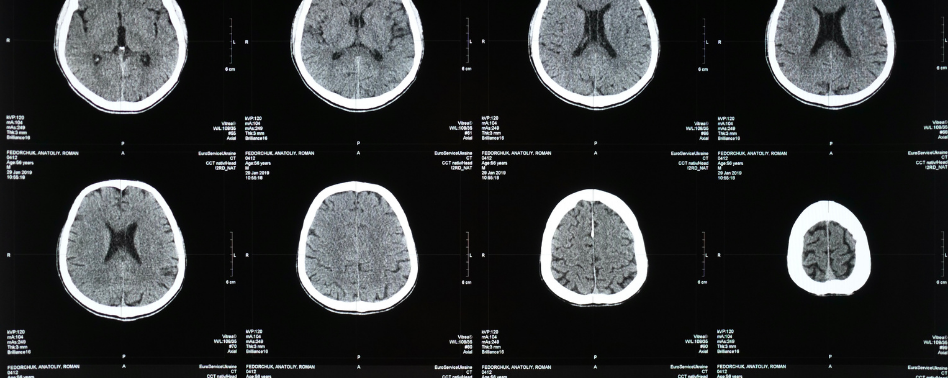
- CT can miss it: Non-contrast head CT is a reasonable start, but up to 50% of scans are normal in PRES, so reassuring early imaging should not end the workup when the syndrome fits.
- MRI confirmation clues: MRI is the most sensitive test, with T2 and FLAIR hyperintensity supporting vasogenic edema; diffusion-weighted imaging helps distinguish PRES from ischemic stroke.
- Named edema patterns: Parieto-occipital edema is the most common pattern, but superior frontal sulcus, holohemispheric watershed, and central variants all occur and can explain atypical presentations.
- Blood pressure strategy: Initial control favors nicardipine or clevidipine with a MAP reduction of 20-25% over the first few hours, while nitroglycerin and nitroprusside are generally avoided.
- Seizure and trigger treatment: Benzodiazepines and levetiracetam are front-line for seizure control, and parallel management means correcting drivers like hypomagnesemia, hypercalcemia, or volume overload.
- Outcome if missed: PRES is often reversible, but delayed recognition can leave up to half of patients with permanent neurologic deficits and carries a mortality around 5-6%. The disposition nuances are worth hearing in the chapter.
Subscribe to ERcast: Clinical Perspectives to listen to the episode.
References:
- Mergen S, Long B, Matlock A. Posterior Reversible Encephalopathy Syndrome: A Narrative Review for Emergency Clinicians. J Emerg Med. 2021 Dec;61(6):666-673. Epub 2021 Oct 23. PMID: 34696929.
Faculty
- Matthew DeLaney, MD, FACEP, FAAEM
Dr. Matthew DeLaney is an emergency medicine physician and educator based in Birmingham, Alabama. A native of Mobile, he earned his medical degree from the University of South Alabama and completed his emergency medicine residency at Maine Medical Center.Dr. DeLaney has experience in both community and academic emergency medicine and is known for his commitment to teaching and medical education. He lives in Birmingham with his wife, Erin, who is also a physician, and their two daughters.
- Brit Long, MD
Dr. Brit Long is a Professor of Emergency Medicine at the University of Virginia and an emergency medicine physician with experience in both a community ED and at a military academic center ED. He is the Clinical Editor-in-Chief of emDOCs.His professional interests include medical education, evidence-based medicine, and the FOAMed movement. Outside of work, he enjoys spending time with his wife and two daughters
